
Egg Freezing
What is Egg Freezing?
Egg freezing, or oocyte cryopreservation, is a process in which a woman’s eggs (oocytes) are extracted, frozen and stored as a method to preserve reproductive potential in women of reproductive age. The first human birth from a frozen oocyte was reported in 1986. Oocyte cryopreservation has advanced greatly over the past few years, with improved overall success of eggs surviving the freezing process. It is no longer considered an experimental procedure by the American Society for Reproductive Medicine. The techniques leading to enhanced gamete survival, potential fertilization and live birth rates allow women a much greater degree of autonomy than was possible even in the past 5 years.
Who needs Egg (oocyte) Freezing?
Cryopreservation of the oocytes can be considered for a variety of reasons:
- Women with cancer requiring chemotherapy and/or pelvic radiation therapy that may affect fertility.
- Surgery that may cause damage to the ovaries.
- Risk of premature ovarian failure because of chromosomal abnormalities (e.g. Turner syndrome, fragile X syndrome), or family history of early menopause.
- Ovarian disease with risk of damage to the ovaries.
- Genetic mutations requiring removing the ovaries (e.g. BRCA mutation).
- Fertility preservation for social or personal reasons to delay childbearing.
How is Egg Freezing Done?
Egg Freezing Process
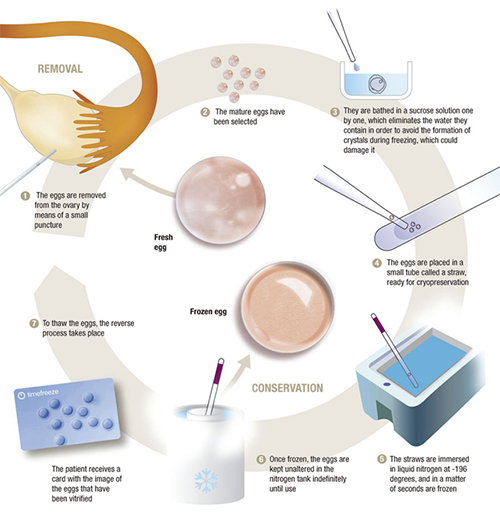
First, your UCLA fertility specialist may perform an assessment of the ovarian reserve to estimate the potential yield of oocytes prior to ovarian stimulation cycle. The assessment would include blood tests and pelvic ultrasound. This will also help to determine the necessary dose of medications. Ovarian stimulation is carried out in the same manner that is used with in vitro fertilization (IVF), using injectable hormonal medications. Following the stimulation, the oocytes and the surrounding fluid in the ovarian follicles are aspirated vaginally while under sedation.
The maturity of the eggs is assessed under the microscope, and those that are mature are cryopreserved. Currently, vitrification is the method of choice for cryopreserving oocytes, and this is achieved by ultra-rapid cooling into liquid nitrogen where they can be stored.
How will the Eggs be used in the Future?
When the woman is ready to use the frozen eggs to achieve pregnancy, these cryopreserved eggs are placed in warming solution and assessed. Those eggs that survived the freezing process are fertilized with intracytoplasmic sperm injection (ICSI), where a single sperm is injected directly into the egg, and the fertilized eggs will grow in culture until the embryo(s) are ready to be transferred into the uterus to achieve pregnancy, typically 3-5 days after fertilization.
What are the chances of a successful pregnancy using Frozen-thawed Oocytes?
Egg Freezing Success Rates
Clinical pregnancy rates have been estimated between 4-12% per oocyte. But since egg freezing is relatively new, more data will be needed to have a better idea on these success rates. In general, the two most important factors in determining the probability of a live birth are the woman’s age at the time of egg freezing and the number of available eggs.
Are there effects on the Offspring Conceived from Frozen-thawed Oocytes?
Available data comparing births resulting from previously frozen oocytes with those from fresh oocytes have not shown an increased risk of congenital anomalies. More long-term data, however, will be needed to further assess these risks.
What are the risks associated with the Oocyte Cryopreservation Procedure?
Egg Freezing Risks
Risks are similar to those associated with ovarian stimulation for IVF, which include small risks of ovarian hyperstimulation syndrome (enlargement of the ovaries and fluid accumulation in the pelvis and abdomen), infection, and bleeding related to the egg retrieval procedure.
How long can the Eggs be Stored?
Storing the eggs for longer durations does not appear to have negative effects. However, data are only available for up to 4 years of storage. It must remembered that older maternal age when carrying a pregnancy is associated with higher risks of pregnancy complications, such as high blood pressure, diabetes, and cesarean section. Most clinics have an upper age limit on when these gametes can be used to achieve pregnancy.
Recent Posts

March 29, 2019

March 29, 2019